Jaw dislocation

Jaw Dislocation
I hadn’t realised that I was using a different technique until I saw a patient in the emergency department with a dislocated jaw, explained what I was going to do, and then reduced her jaw in a few seconds. She had previously had a number of painful distressing experiences with her jaw and insisted that I teach other doctors what I had just done to her. So, here is the technique that I use, based on the anatomy of the jaw in dislocation, and using positioning, leverage, and minimal force to reduce the joint.
The clinical picture used here is with the kind permission of Shanti Landon
Click below for a clinical demonstration of the technique

Clinical presentation
The patient usually presents with the jaw locked in the open position, following excessive mouth opening (yawning, laughing etc). The dislocation can be unilateral or bilateral. Any impact to the jaw should raise concern of a concurrent fracture.

Anatomy
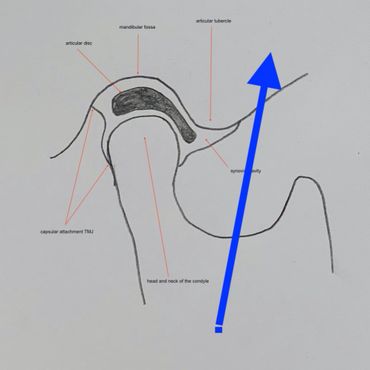
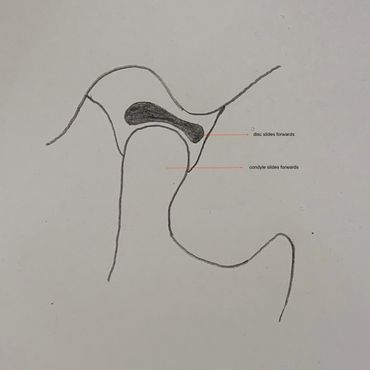
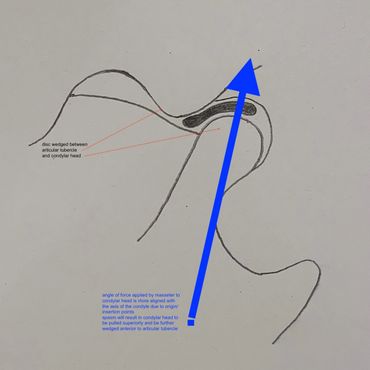
In the Xray the down arrow points to the mandibular condyle, the up arrow denotes the articular tubercle. There is an articular disc that sits between the two. Normally the condyle lies in the fossa when the mouth is closed and moves forwards slightly when open (see pics below). The anatomy in dislocation changes - excessive opening can result in more anterior movement of the condyle which then slips forwards over the tubercle and becomes wedged in position. The pain caused by stretching of the articular capsule causes spasming of the internal pterygoid, masseter and temporalis, which pull the condyle superiorly, further wedging it anterior to the tubercle. Attempting to overcome these spasming muscles with force will result in pain, using force to overcome the obstructing tubercle may result in further injury to the structures.
Closed mouth, open mouth, and dislocated TMJ position
my technique

My approach
This is designed to ease the condylar head back onto the articular tubercle and then angle it backwards, allowing it to slide back behind the tubercle. Pulling down will simply activate further spasm of the aster and be counter-productive resulting in an upwards pull of the head.
stand in front of seated patient
- double gloved thumbs placed firmly but gently behind lower molars.
- “hold.” This steady and very gentle pressure is maintained throughout to act as a fulcrum holding the condyle against the articular tubercle during reduction movement. This is absolutely not to pull against or attempt to overcome muscular spasm (attempting to overcome the muscle spasm is not a good idea)
- little fingers of both hands placed under the mental process of the chin which is slowly lifted in order to allow the articular surface of the mandibular condyle to roll over the disc overlying the articular tubercle.
- once the chin is lifted to an appropriate angle the condyle will slide posteriorly back into the mandibular fossa.

Step by step
- stand in front of seated patient
- thumbs placed firmly but gently behind molars - a "hold"
- steady gentle pressure maintained throughout to act as a fulcrum - do not push down
- little fingers of both hands placed under chin (mental process) which is slowly lifted

Big hands, I know you're the one....
One of my registrars discovered that her hands were too small to allow her little fingers to lift the chin, easily solved by me doing that part for her, lifting the chin with my index finger. If you discover that issue while positioning your patient, grab an assistant.
Yawning tip for your patients

How to yawn
For patients with jaws that dislocate on excessive mouth opening I always tell them how to yawn. Yawning is a fascinating phenomenon with the urge to yawn triggered by seeing other humans do so or even reading about it (you probably feel like yawning just reading this). The urge to yawn especially when tired is strong and saying "don't yawn" is not realistic but if it may result in a dislocation then there is a problem. Keeping the tongue connected to the roof of the mouth while yawning allows the yawn to occur (scratching that neurological itch) but keeps the mouth at a safe level of closure, stopping the precarious anterior movement of the condylar head. Try a yawn now, you know you want to.
I met him in an ice bar in downtown queenstown

A couple of years ago I was at the ACEM conference in Queenstown, New Zealand and was introduced to a guy called Rich who used my shoulder technique (badly as the photo proves!) When I told him I also used a jaw technique he made me promise to put it online so this one's for you, Rich. We were in an ice bar at the time and bring to explain where your thumbs go while wearing massive gloves and drinking cocktails is not easy. You can check out Rich at @airwaycam or better still, get onto one of his great airway courses.