proximal tibiofibular joint dislocation

Clinical Presentation
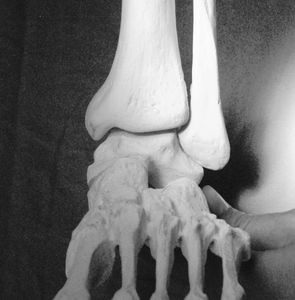
Isolated PTFJ dislocations are rare, accounting for less than 1% of all knee injuries. Once dislocated, the fibular head sits in an anterolateral position, with the anterior surface of the superior tibia directly behind.
The mechanism most commonly follows a fall with the following anatomical positions occurring at the point of dislocation – ankle inversion, foot plantar flexed, and knee flexed or hyper-flexed
A tender deformity appears at the proximal fibula area, the knee usually held in full extension.

Technique
Click below for a clinical demonstration of the technique being performed on a patient. At the bottom of this page is a case report and review article with additional detail on the technique and underlying anatomy (with thanks to my co-authors Nick and Jake!)

Imaging
A number of case studies have demonstrated the risks of misdiagnosis with unilateral lower limb imaging so do bilateral knee imaging to allow direct comparison.
CT may be needed in cases with inconclusive x-ray findings and those of suspected fractures.
Proximal tibio-fibular joint dislocation

Anatomy in dislocation
Once dislocated, the fibular head sits in an anterolateral position, with the anterior surface of the superior tibia directly behind. From this position, the head must travel inferiorly, laterally, posteriorly and then medially in order to reduce.
Obstacles to reduction
- The flared lateral aspect of the superior tibia, which provides a bony posterior obstacle. This posterior obstacle is reduced inferiorly due to the shape of the tibia.
- Tension of the lateral collateral ligament and biceps femoris tendon. These stop the descent of the fibular head, and pull the head superiorly and against the anterior surface of the tibia.
- The ankle is no longer in an exaggerated inversion/plantar flexion, so the ability of the distal fibula to move inferiorly is impeded.
- The knee is no longer flexed, resulting in further lateral collateral ligament tension.

Step-by-step technique
Sedate patient
Place ankle into inversion and plantar flexion
Flex knee to 90 degrees
Apply downward pressure to the fibular head, which can then be guided laterally and posteriorly if required
What's up Nick?

Necessity is the mother of creation!
I’d never seen a proximal fibula dislocation until Nick Farebrother @Apostalidis came through to the main area of the emergency department and said “come and see this guy, I think he’s dislocated his fibula!” Nick is one of our nurse practitioners and very much a gun where it comes to musculoskeletal pathology so had already organised for bilateral X-rays to confirm his suspicion, and done a background search on the injury. There wasn’t a reduction technique so I worked out the dislocation anatomy and came up with a plan by the time the patient was back from X-Ray. This is why I love emergency medicine, just when you think you’ve seen everything, an unusual case will come through the door that forces you to be creative and problem solve in real time!
review article: isolated PTFJ dislocation